The incidence rate of cancer had risen for both males and females during the period between 1968-1972 and 2014-2018 in Singapore (Singapore Cancer Registry Annual Report 2018).
In our country, lung cancer is in the top three incidence of cancer for both male and female. It is the number one in cancer death among the males and the second leading cause of death among females from 2014-2018.
Lung cancer is among the three most frequent cancers in males for all the three ethnic groups: Chinese, Malays and Indians. In 2013-2017, Malay males overtook Chinese males to be the ethnic group having the highest ASIR (Age Standardised Incidence Rate). However, the ASIR was consistently the highest among Chinese females in the past fifty years, and lowest among Indian females.
Lung cancer incidence rates were two times higher in males compared to females. This was most likely related to the smoking prevalence rates.
The risk of developing lung cancer increased sharply with age. It was fourth (8%) in age group 40-49, second (11.7%) in 50-59, third (13.7%) in 60-69, second (16.9%) in 70-79 and first (18.4%) in 80+ age group for males. As for females, it was third from 60 years old and above.
Types of Lung Cancer
There are two major types of lung cancer: small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC). SCLC makes up 10-15% of all lung cancer. It is aggressive and grows quickly and spreads early to other parts of body. It is strongly associated with cigarette smoking. NSCLC is not so aggressive but more common. It includes squamous cell carcinoma (25-30%), large cell carcinoma (10-15%) and adenocarcinoma (40-50%).
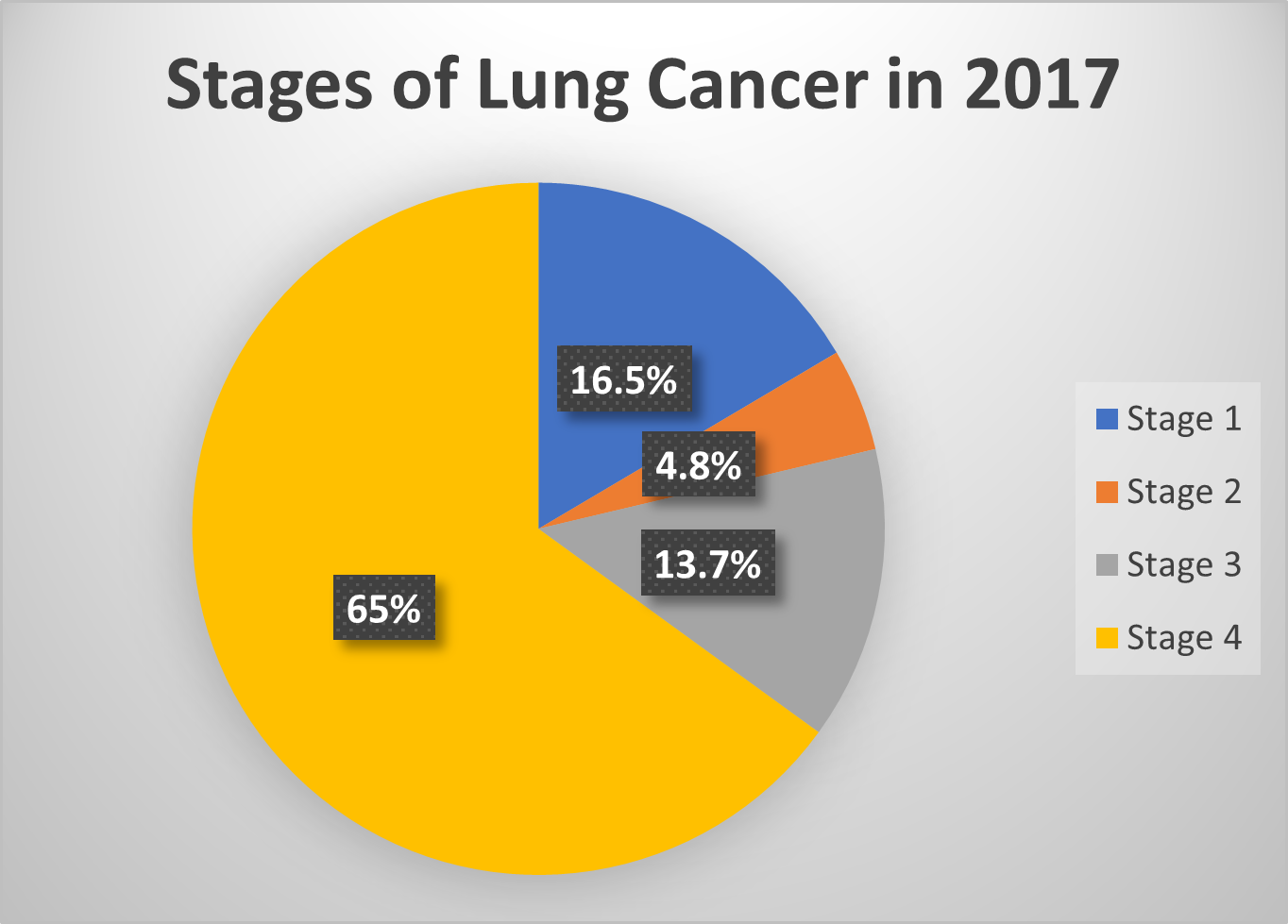
Stage at Diagnosis
The overall survival rate for lung cancer patients was poor especially for males. This was because most of the cases were diagnosed at advanced stage, about two thirds were diagnosed at Stage IV in the past decade. The pie chart shows the stage distribution of lung cancer in Singapore in 2017, 65% in stage 4 at diagnosis (50 years of Cancer Registration 1968-2017, Singapore Cancer Society). The five-year ASRS (Age-standardised Relative Survival) was much lower for cases diagnosed at Stage 4 in 2013-2017 (less than 10%) compared with cases diagnosed at earlier stages (1-2) in the same period (above 35%).
Risk factors for Lung cancer:
Cigarette smoking: the number one risk factor and is increased with the number of cigarettes smoked and the duration of smoking. The risk is 15-25 times more than a non-smoker. Former smokers still have a higher risk of lung cancer than people who never smoked
Second-hand smoking or passive smoking: the main risk factor among non-smokers
Age: incidence is related to age, with higher incidence rates amongst the older men and women
Exposure to Cancer causing chemicals: asbestos, coal gas, chromates, nickel, arsenic, vinyl chloride, mustard gas, cadmium, beryllium and radon
Personal or family history of Lung Cancer: lung cancer survivor might have a risk to develop another lung cancer especially in the smokers, and risk may be higher if parents or siblings or children have had lung cancer
Pulmonary Fibrosis and Chronic obstructive pulmonary disease
At the early stage, there may not be any symptoms of lung cancer. The common symptoms include:
- General weakness, tiredness and unexplained weight loss
- Persistent and progressive cough
- Blood in the sputum
- Shortness of breath
- Recurrent Lung infection
- Wheezing
- Hoarseness
- Constant chest pain
- Symptoms from metastases like enlarged lymph nodes
How is Lung Cancer Diagnosed by your Lung Specialist?
The diagnosis is made using one or more of these tests:
- History and physical examination
- Chest X-ray
- Bronchoscopy and EBUS biopsy of mediastinal and hilar nodes
- Imaging studies: CT scan and PET scan
- Transthoracic needle biopsy
- Mediastinoscopy or video-assisted thoracoscopic surgery
Staging of Lung Cancer
The severity of the Lung Cancer is measured by the stage of the disease and indicates how far the cancer has spread:
| Stage |
Extent of Spread |
5 years ASOS (Males) |
5 years ASOS (Females) |
| 1 |
Cancer confined to the lung and surrounded by normal tissue |
54% |
69% |
| 2 |
Cancer has spread to nearby lymph nodes |
33% |
45% |
| 3 |
Cancer has spread to the chest wall, diaphragm, nearby organs, blood vessels, lymph nodes in the mediastinum or the other side of the chest or neck |
11% |
20% |
| 4 |
Cancer has spread to more distant sites in the body |
3% |
5% |
ASOS-Age-Standardised Observed Survival Rate
Source: Singapore Cancer Registry Annual Registry Report, Trends in Cancer Incidence in Singapore (2010-2014)
Treatment Options
Patients with lung cancer that is detected early (Stage 1 and 2), surgery is recommended. This may be followed by chemotherapy. However, for patients with lung cancer that has already spread beyond the lung, chemotherapy is one option and it may be combined with radiotherapy. For those whose lung cancer has specific genetic mutations, targeted therapy using drugs that block these specific mutations are very effective in controlling the cancer. Immunotherapy, which harnesses the patient’s own immune system to fight cancer has also shown to benefit certain patients
Why screen for Lung Cancer?
Most lung cancer is found after symptoms appear, when it may be too late to treat or cure. So, the goals of screening are:
- Find cancer before symptoms start
- Find cancer at an early stage when it is easier to treat and cure
- Reduces chance of dying from cancer
Lung cancer screening is not part of our National Cancer Screening Programme. However, they recommend targeted screening through low dose CT scans of the lung for high-risk individuals:
- Adults aged 55-80 years
- 30 pack-year smoking history (For example: a pack a day for 30 years, 2 packs a day for 15 years)
- Current smokers
- Smokers who quit within the past 15 years
These are based on two major studies: The US National Lung Screening Trial (NLST, 2011) and Dutch-Belgian NELSON Trial (2020). The former compared Low Dose CT (LDCT) with chest x-ray (CXR) in lung cancer screening and the latter compared LDCT with no screening. Both trials recruited heavy smokers and LDCT detected more lung cancers at earlier stages. The NLST showed a 20% reduction in lung cancer mortality with LDCT screenings. The NELSON trial demonstrated reduction in lung cancer mortality with LDCT screening both among men (by 24%) and among women (by 33%).
K-LUCAS (2019) is the first Asian population-based, nationwide, multi-centre prospective lung cancer screening trial in South Korea. The results were promising as the proportion of early-stage lung cancer detection was three times higher in K-LUCAS than early-stage lung cancer cases in the national cancer registry. Lung cancer incidence in never-smokers has been increasing rapidly in Korea. However, the screening has not been extended to this group.
TALENT (2021) a national lung cancer screening study conducted in Taiwan uncovered the presence of lung cancer in 2.6% of the study population, exceeding the 1.1% and 0.9% lung cancer detection rates documented in NLST and NELSON respectively. This study was conducted in high risk never-smokers as opposed to heavy smokers in the previous two studies. Lung cancer is the leading cause of cancer -related mortality in Taiwan and 53% of these deaths occurred among never-smokers. The study involved individuals aged 55-75, normal chest x-ray and any of the following high-risk features: family history of lung cancer, environmental smoking exposure, history of chronic lung disease like tuberculosis or chronic obstructive pulmonary disease, cooking without ventilation. 73.8% of the study population were women. 96.5% of the patients were diagnosed with stage 0 or 1 disease, providing opportunity for curative resection. All lung cancer identified except for one were adenocarcinomas. The highest risk factor among these never-smokers was family history of lung cancer and the more first-degree relatives with lung cancer, the higher the likelihood of detection. LDCT lung cancer screening for never-smokers with high risk may be feasible but long-term data are needed to determine whether screening these individuals leads to lower lung cancer mortality.
In Singapore, there is also a higher proportion of non-smokers diagnosed with lung cancer 47% compared to the West (10%). In addition, there is also greater incidence of adenocarcinoma, 77.6% in Singapore compared to 38.5% in US particularly in women. This represents a distinct disease in Asia. The genomic profile, the carcinogenesis and pattern of progression seem different. Screening in this group is not established. Should we use the TALENT criteria? Screening in the meantime should be individualised. The younger age group should not be excluded if they have any risk factor.
False positive is a concern in screening. They tend to lead to further tests and procedures potentially causing more anxiety and increasing costs. This is in addition to the risk of radiation. Please consult your lung specialist for a discussion on the risks and benefits of screening.
Lifestyle and behavioural factors such as obesity, physical inactivity and smoking increases an individual’s risk of developing cancer. As such, it is important to encourage healthy behaviour to minimise the impact of these risk factors. Do your best to avoid these preventable factors.